


Assessment of Quality of life (QoL) in postmenopausal osteoporosis in the Lublin region
-
Copyright
© 2016 PRO MEDICINA Foundation, Published by PRO MEDICINA Foundation
User License
The journal provides published content under the terms of the Creative Commons 4.0 Attribution-International Non-Commercial Use (CC BY-NC 4.0) license.
Authors
| Name | Affiliation | |
|---|---|---|
Mariola Drozd |
Department of Applied Pharmacy, Medical University of Lublin |
|
Joanna Mazur |
3 Department of Child and Adolescent Health, Institute of Mother and Child, 17a Kasprzaka str., 01-211 Warsaw, Poland |
|
Monika Szkultecka-Dębek |
Department of Dermatology, Military Institute of Medicine, 128 Szaserów str., 04-141 Warsaw, Poland |
|
Lucyna Bułaś |
School of Pharmacy with the Division of Laboratory Medicine in Sosnowiec, Department of Applied Pharmacy, Institute of Pharmaceutical Technology, Medical University of Silesia in Katowice, 3 Kasztanowa str., Sosnowiec, Poland |
|
Maria Jesiotr |
Department of Applied Pharmacy, Medical University of Lublin, 1 Chodźki str., 20-093 Lublin, Poland |
|
Rafał Filip |
Medical Department, University of Rzeszów, 16c Rejtana str. 35-959 Rzeszów, Poland |
Introduction: Postmenopausal osteoporosis is related to the changes in female body during menopause. The aim was to assess the quality of life of women in the Lublin region suffering from postmenopausal osteoporosis.
Methods: Data was obtained from standardized osteoporosis QoL questionnaire – Qualeffo-41. The survey was conducted in April 2013 in a group of women with postmenopausal osteoporosis treated in ambulatory setting.
Results: In total 55 QoL questionnaires were collected. The mean age was 70 years. The last declared menstruation was between 40 and 56 years. City inhabitants included 41 women, while 14 women inhabited rural areas. There were 28 married women, 25 widows and 2 maidens. The respondents’ weight was between 42 - 102 kg. The shortest subject was 147 cm tall and the tallest - 170 cm.
The results of QoL were at 49.38. The results of the individual domains of the questionnaire indicate that the lowest rating was for physical function – mean of 39.41. Mental functions were assessed on average at 53.03. Pain assessment resulted on average at 53.45. The functioning during free time and opportunities for social contact were rated on average at 56.66. The highest result was for overall health with a mean value of 79.55.
Conclusion: The analysis showed that Polish women suffering from postmenopausal osteoporosis have a low quality of life. The results suggest further research to test QoL at the beginning of the therapy and to monitor it during treatment, analyzing the domains that need the most improvement.
Background
Menopause can be defined as a period of transition from a reproductive period to the advanced age. This period is characterized by hormonal changes in the female body which are associated with different diseases and symptoms. Due to their influence the quality of life as well as the interactions with the environment can deteriorate. Many women begin to develop diseases such as obesity, hypertension, diabetes and osteoporosis [1,2].
Osteoporosis as defined by the World Health Organization (WHO, 1994) is ”skeletal systemic disease characterized by low bone mass, microarchitectural deterioration and fragility” and “a bone density 2.5 standard deviations below the mean for young white adult women at lumbar spine, femoral neck or forearm” [3]. In 2001, the National Osteoporosis Foundation (NOF) and the National Institutes of Health in the USA developed a different definition describing osteoporosis as "a skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture" [4]. In 2013 Clinician's Guide to Prevention and Treatment of Osteoporosis was developed. In this Guide NOF in collaboration with experts from different fields of medicine indicate the latest advice on prevention, risk assessment, diagnosis and treatment of osteoporosis in postmenopausal women and men over the age of 50 years. According to the authors of the guide osteoporosis is “a silent disease until it is complicated by fractures—fractures that occur following minimal trauma or, in some cases, with no trauma” [5]. In 2014 Polish guidelines were compared with other international guidelines in terms of diagnostic measures, pharmacotherapy and calcium and vitamin D supplementation [6]. Depending on the cause of osteoporosis development we can differentiate primary and secondary osteoporosis. Most frequent (80%) is the primary disease and can be idiopathic or involutional. The idiopathic form is rather rare and usually affects young people without a known cause. The involutional form can be postmenopausal or senile. The form we predominantly observe is the postmenopausal type (80%) [7,8].
Osteoporosis is considered to be a social disease because of the incidence of the disease and the consequences. It is estimated that, due to complications within six months after the fracture of the femur, 20% of patients die and 50% die within the next year. It is estimated that since the number of hip fractures in 2000 was 1.6 million cases worldwide, then in 2025 it may reach 4 million, and in 2050 even 6 million [7, 9]. These fractures cause patient’s immobilization, loss of independence and pain which results in reduction of the quality of life [10]. More than 30% of the vertebral body fractures do not cause clinical symptoms [11]. However all the other patients feel persistent pain and that affects significantly their quality of life [7].
Epidemiological data from 2008, related to Poland indicate that among people over 50 years, 165/100 000 are experiencing osteoporotic fracture. In case of people over 85 years of age, the figure is 666 for men and 1 138 for women per 100 000/year [9]. A study conducted in a Podlasie region showed that the proportion of women with fractures and without them at different ages, among whom a history of osteoporotic fractures occur in the 5th decade of life is reported in 20%, in the 6th - 16.8%, in the 7th - 29.2 % , in the 8th - 33.5%, and in the 9th decade – 44.4%. On average, in the whole population 27% of the women experienced in the past low-energy fractures [12]. In other study conducted in Poznan it was demonstrated that 40% of respondents after a fracture rated their quality of life as poor. Prior to the trauma, 8% of patients assessed their QoL as bad, while all the respondents consistently complained about a significant deterioration in relation to pain [13].
The aim of this study was to assess the quality of life in postmenopausal women suffering from osteoporosis. In addition, an attempt was made to verify the correlation between the place of residence, age, BMI, the occurrence of fractures and quality of life of patients.
Material and Methods
In recent years, it has been proven that there are needed questionnaires measuring health status for the research purposes and for clinical practice as well. The questionnaires are based on health status variables, such as mood, physical and social functioning and patient self-management. The general scales to measure health status are used to evaluate patients suffering from various diseases, however these scales are not measuring specific functioning in a given disease. Therefore it was necessary to construct a specific scale for osteoporosis. The questionnaire which is recommended by the International Osteoporosis Foundation (IOF) [14] is the called Quality of Life Questionnaire of the International Osteoporosis Foundation (Qualeffo-41) [15]. The questionnaire consists of 41 questions in the following 5 subscales: pain (5 questions), physical function (17 questions), social function (7 questions), general health perception (3 questions) and mental function (9 questions). When filling out questionnaires only one answer to each question should be selected. For the total score and subscores, “0” indicates a good health status, whereas “100” indicates a poor health status [16].
The studied material consisted of data of the interview conducted by the appropriately trained interviewer. The interviews were conducted among 55 patients undergoing a medical treatment at the clinic for osteoporosis treatment in April 2013. The interview included a questionnaire Qualeffo-41 with the addition of a special copyright questionnaire to characterize the studied group of patients. This additional questionnaire allowed us to collect information about age, weight, height, age of onset of the last menstrual period, the concomitant diseases and history of bone fractures. The interview lasted on average 25-30 minutes. The study was conducted at two clinics treating osteoporosis in Lublin. There was a random selection of the studied group, which included women aged 54 - 86 years, average 70 years (median 72 years). The age distribution of women in the study group is shown in Figure 1. The inclusion criterion was a history of menopause and osteoporosis diagnosed by the patient declared verbally and its written consent to participate in the study. The obtained data were compiled using MS Office Excel 2007, and the results are presented as descriptive statistics and as figures and tables. For the purpose of the statistical analysis the significance index and Pearson correlation and the index α-Cronbach were used. The assumed level of statistical significance was α = 0.05. The study received a positive opinion of the Bioethics Committee of the Medical University of Lublin.
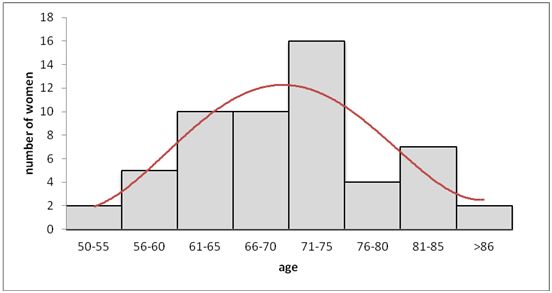
Figure 1. The number of women in the different age groups
Results
Taking into account 55 patients, it should be pointed out that they represented a diverse population of patients with postmenopausal osteoporosis. The assessment of the demographic data of women surveyed is shown in Table 1.
Table 1. Socio-demographic characteristics of women with postmenopausal osteoporosis
|
characteristic |
Patients N=55 |
|
|
Place of residence
Marital situation
Weight
Height
Body mass index (BMI)
Age at menopause
Fracture
coexisting diseases |
Urban Rural Married Widowed Single Mean Median Mean Median Mean Median SD Mean Median SD Yes No Yes No |
41 (74.5%) 14 (25.5%) 28 (50.9%) 25 (45.5%) 2 (3.6%) 62 kg 60 kg 158 cm 160 cm 24.7 23.8 4.2 49 years 50 years 4.0 21 (38.2%) 34 (61.8%) 42 (76.4%) 13 (23.6%) |
The fractures declared by women usually concerned the lower limbs (12 persons, 21.8%), including: ankle (3 people, 5.45%), the hip bone (1 person, 1.8%), the toes (3 women, 5.45%). Fractures of upper limbs were reported by12 people, representing 21.8% of the respondents, including: wrist (5 people, 9.1% of respondents), shoulder (2 women, 3.6% of respondents). Broken ribs was reported by 1 person (1.8% of respondents). Vertebral fractures were experienced by 2 people (3.6% of respondents). Broken collarbone was reported by 1 person (1.8% of respondents).
Patients also reported concomitant diseases: hypertension, neurological diseases, thyroid disease, rheumatoid arthritis, gallstones, or kidney stones, glaucoma and cataracts.
In the first step, we analyzed the psychometric properties of the questionnaire Qualeffo-41 in the sample of 55 women. According to the analysis of reliability, four of the five dimensions of Qualeffo-41 questionnaire have good psychometric properties as α-Cronbach ratio significantly exceeds the 0.7, which is considered as the threshold value. The best result concerns the physical functioning domain. The α-Cronbach value below 0.7 was obtained for measuring mental functioning. The properties of this subscale are significantly improved by the elimination of question # 38 (Do you get annoyed by details?).
Table 2. Description and reliability of Qualeffo-41
|
Domain |
No of items |
Description |
Cronbach α |
|
Pain |
5 |
Back pain; Sleep disturbance |
0.792 |
|
Physical function |
17 |
Activities of daily living; Jobs around the house; Mobility; Walking outside |
0.918 |
|
Social activities |
7 |
Sport; Gardening; Hobby; Theatre; Visiting friends; Intimacy |
0.812 |
|
General health perception |
3 |
General health; overall quality of life; Change in quality of life |
0.867 |
|
Mental function |
9 |
Fatigue; Depression; Loneliness; Energy; Hopefulness; Fear of becoming dependent |
0.628 |
The evaluation of the quality of life of women with postmenopausal osteoporosis was based on a standardized questionnaire Qualeffo-41. The results are summarized in Tables 3 and 4.
Table 3. Results of quality of life measured with Qualeffo-41
| Statistics | Total | Qualeffo-41 domains | ||||
| Pain | Physical function | Social activities | General health perception | Mental function | ||
| Mean | 49.38 | 53.45 | 39.41 | 56.66 | 79.55 | 53.03 |
| Median | 51.16 | 55.00 | 38.24 | 61.43 | 83.33 | 52.78 |
| Minimum | 12.80 | 0.00 | 7.35 | 0.00 | 33.33 | 19.44 |
| Maximum | 80.00 | 90.00 | 80.88 | 90.00 | 100.00 | 80.56 |
| SEM | 1.46 | 2.40 | 1.69 | 2.35 | 1.80 | 1.36 |
| 95% CI | 2.86 | 4.70 | 3.31 | 4.61 | 3.52 | 2.66 |
It should be noted that the overall average quality of life of women surveyed is 49.38 (SEM 15.46). However, in various domains of the questionnaire it was found that women assessed the overall health as the worst with an average of 79.55 (SEM 1.80). There was even recorded a maximum value in case of 17 people, i.e. “A very bad condition”. The next step was to assess the functioning during free time and opportunities for social contact, rated on average at 56.66 (SEM 2,35) at the lowest value of 0.0 in 2 patients, which can be explained as a lack of disruption in social activities and the highest of 90 in case of 4 women for whom the assessment has shown great difficulty in social activities. “Feeling pain”, was another domain with an average score of 53.45 (SEM 2.40). In this case, the lowest value - 0.00 was observed in 5 women, which indicates the lack of pain, as well as the highest value recorded here was 90.00 in 3 women, which is a significant perception of pain. The surveyed women found mental functions on average at 53.03 (SEM 1.36), with the best value 19.44 (1 woman) and the worst 80.56 (3 women). However, despite significant pain, women gave the best rating in physical function - the average value is 39.41 (SEM 1.69), which means that surveyed women had not significant difficulties in the physical functioning in relation to movement.
Table 4. The average indexes of quality of life assessed by questionnaire Qualeffo-41 and selected characteristics of patients with osteoporosis
|
|
|
Total |
Qualeffo-41 domains |
||||||
|
Pain |
Physical function |
Social activities |
General health perception |
Mental function |
|||||
|
Place of residence |
|||||||||
|
Urban |
Mean |
49.49 |
55.98 |
39.96 |
56.44 |
78.86 |
51.76 |
||
|
SD |
14.09 |
21.89 |
17.38 |
23.64 |
18.36 |
13.90 |
|||
|
Rural |
Mean |
48.60 |
46.07 |
37.82 |
57.30 |
81.55 |
56.75 |
||
|
SD |
18.98 |
32.83 |
19.18 |
29.79 |
20.72 |
15.13 |
|||
|
p |
|
0.929 |
0.327 |
0.808 |
0.933 |
0.832 |
0.632 |
||
|
Marital status * |
|||||||||
|
married |
Mean |
42.35 |
45.18 |
32.88 |
44.76 |
74.70 |
49.90 |
||
|
SD |
15.56 |
28.72 |
17.12 |
26.98 |
18.21 |
13.62 |
|||
|
widow |
Mean |
57.19 |
63.20 |
47.12 |
70.24 |
85.67 |
56.22 |
||
|
SD |
11.49 |
17.37 |
16.16 |
15.15 |
18.71 |
14.73 |
|||
|
p |
|
0.137 |
0.083 |
0.111 |
0.018 |
0.386 |
0.540 |
||
|
Age (years) |
|||||||||
|
50-60 |
Mean |
23.91 |
20.71 |
14.50 |
15.95 |
60.71 |
38.49 |
||
|
SD |
9.22 |
29.64 |
5.46 |
19.07 |
15.75 |
11.83 |
|||
|
61-70 |
Mean |
47.08 |
51.84 |
37.69 |
51.86 |
77.63 |
50.88 |
||
|
SD |
11.59 |
26.36 |
16.33 |
20.43 |
16.45 |
12.32 |
|||
|
71 and older |
Mean |
56.82 |
62.41 |
46.55 |
69.63 |
85.34 |
57.95 |
||
|
SD |
11.11 |
15.27 |
14.71 |
16.14 |
18.18 |
13.52 |
|||
|
p |
|
0.001 |
0.000 |
0.000 |
0.000 |
0.119 |
0.139 |
||
|
Body weight ** |
|||||||||
|
BMI 18.5 – 24.99 |
Mean |
48.89 |
53.86 |
38.40 |
55.14 |
80.48 |
53.81 |
||
|
SD |
16.53 |
27.20 |
18.83 |
25.93 |
19.49 |
14.68 |
|||
|
BMI 25.0 – 29.99 |
Mean |
50.03 |
53.57 |
42.02 |
59.32 |
75.60 |
52.18 |
||
|
SD |
11.73 |
21.34 |
15.14 |
20.33 |
18.91 |
13.13 |
|||
|
BMI 30> |
Mean |
45.39 |
51.00 |
35.29 |
53.15 |
80.00 |
44.44 |
||
|
SD |
15.79 |
27.70 |
17.98 |
32.85 |
15.14 |
7.61 |
|||
|
p |
|
0.886 |
0.954 |
0.745 |
0.837 |
0.912 |
0.607 |
||
|
History of fractures |
|||||||||
|
yes |
Mean |
56.13 |
59.29 |
46.08 |
66.73 |
84.52 |
59.39 |
||
|
SD |
12.41 |
26.33 |
16.15 |
16.64 |
16.31 |
12.95 |
|||
|
no |
Mean |
45.03 |
49.85 |
35.29 |
50.44 |
76.47 |
49.10 |
||
|
SD |
15.52 |
24.10 |
17.57 |
27.48 |
19.83 |
13.74 |
|||
|
p |
|
0.270 |
0.366 |
0.232 |
0.132 |
0.526 |
0.323 |
||
* Due to small number single women were not included into calculations** Due to small number of patients with BMI <18.5 not included into calculations
Correlation between the assessment of the quality of life with the place of residence, age, marital status, BMI and a history of fractures indicated that there was no statistically significant difference in case of analysis in relation to place of residence, marital status, BMI and a history of fractures. Statistically significant differences were demonstrated in the analysis in relation to age and for marital status in the social activities domain. It was found that with age the quality of life should deteriorate, which results in a longer life with the disease. This study confirms that hypothesis. For the pain domain depending on the marital status, the value of calculated p is at borderline of statistical significance.
We also decided to analyze the correlation between the five domains of the questionnaire. The results are summarized in Table 5. Correlation coefficients range from 0.325 to 0.655, assuming that the highest value of correlation is for physical function and social activities. Also it is worth to pay attention to the high correlation (r = 0.610) between the two domains, which are more than any other domain for osteoporosis (pain and limitations in functioning).
Table 5. The correlation matrix between the five dimensions of the questionnaire Qualeffo -41
|
|
Pain |
Physical function |
Social activities |
General health perception |
Mental function |
|
Pain
|
1 |
0.610 |
0.522 |
0.421 |
0.325 |
|
Physical function |
0.000 |
1 |
0.655 |
0.591 |
0.558 |
|
Social activities |
0.000 |
0.000 |
1 |
0.472 |
0.357 |
|
General health perception |
0.001 |
0.000 |
0.000 |
1 |
0.608 |
|
Mental function |
0.016 |
0.000 |
0.008 |
0.008 |
1 |
*In the top of the table is the Pearson correlation coefficient, in the lower its significance
Discussion
Quality of life as defined by the World Health Organization, is an individual perception of their position in life, taking into account cultural conditions and a system of values in relation to individual objectives, standards, expectations and problems. QoL studies, in particular for diseases that cause an increase in pain suggest that such diseases significantly affect the deterioration of the mental and physical dimensions of quality of life [17].
A survey of one hundred postmenopausal women, aged 66 ± 8.7 years (age range 50-85), affected by osteoporosis with / or without fractures, done by the surgery clinic of the Instituto Italiano Auxologico for a period of about 4 months has shown that pain was present in 50% of cases and in 26% for more than 10 hours per day [18] . In the studies carried out in this work pain was present in 89%. The pain lasted 1-2 hours per day at 32.7%, 3-5 hours in 12.7%, and 6-10 hours at 3.6% of patients. Back pain lasting the whole day occurred in 40% of patients.
In a study conducted at the clinic Instituto Italiano Auxologico, in the area of physical fitness, 46% of women under 65, and also 65% of people over 65 years declared significant changes [18]. For Polish women getting up from the chair causes difficulties in case of 62% of patients, bends - 64%, kneeling – 67%, walking up the stairs – 93%, walking 100 meters – 51%.
In the category of general health perception, according to a study in Italy, 58% of the women had poor well-being. In 21% of the 62 women, a reduction of their health perception was reported. Comparing their current level of health status with that of 10 years before, 58% of women aged below 65 indicate a deterioration, similarly as 83% of people aged 65 or more. Reduced quality of life was confirmed by 41% of women affected by osteoporosis [18]. According to research conducted for this study, most of the patients identified their health as fair - 36.4% or poor - 36.4%. In contrast, 21.8% described it as satisfactory. Most of the patients identified their overall quality of life as satisfactory (40%) and poor (34.5%). None of the patients defined quality of life as excellent. Satisfactory quality of life was reported by 34.5%. Comparing their current level of wellbeing with that of 10 years before, 91% of patients indicated its deterioration. In a study conducted in an Italian clinic, it was estimated that 40% of surveyed women had symptoms of depression [18]. According to our survey 100% of patients were experiencing fatigue. Also, as in the Italian study, we can conclude that approx. 40% of women have symptoms of depression, because they feel depressed, lonely, and only 40% of respondents thought indicated “only sometimes with hope on the future” response.
Papaioannou, A. et al. believe that the experience of osteoporotic fracture has a negative impact on patient quality of life. The factors that play the biggest role is pain and disability, the ability to self-care and mobility [19,20]. Osteoporotic fractures lead to a reduction of efficiency and reduced quality of life and are associated with increased mortality. Because of the pain, impairment of movement and limitation in self-care activities, during the first months of the injury occur and a significant deterioration in QoL regardless of the location of the fracture [20]. The study by Abimanyi-Ochom J. et al. conducted using the EQ-5D questionnaire, found the average decrease in QoL for all fracture locations. Immediately after the injury decrease at an average of 51%, the largest decrease was recorded in the proximal femur fracture 69%, least (36%) of the radius bone. In the case of proximal femur and vertebral fractures, QoL did not return to the level from before the event even after 18 months, with 83- 89% of the initial value [20,21]. In the Swedish study using the same protocol, O. Ström et al. obtained similar results [20,22]. The study in Lublin confirms the results obtained by A. Papaioannou, J. Abimanyi-Ochom and O. Ström et al. Polish women with osteoporotic fractures have reduced QoL.
In the Outpatient Treatment of Osteoporosis and Menopause and Orthopedic Clinic in Poznan, among 100 women aged 50 to 70 years (research carried out for 11 months), a study was conducted to assess the quality of life of women suffering from osteoporosis. The women were divided into 3 groups. The first group consisted of women with osteoporosis, the other with osteopenia, and the third one of healthy women. Worse functioning was demonstrated in women with osteoporosis in the field of performing daily activities, mobility, leisure activities and opportunities for social contact. The first group of women received the best results in the field of mental functioning [23]. This study confirms the results obtained in Poznan. The research of Bianchi et al. showed that 58% of women with osteoporosis assess the overall state of their health as low. The reduced quality of life is reported by 41% of women suffering from osteoporosis. Patients suffering from osteoporosis have a more depressed mood and lower quality of life compared to healthy subjects [18]. The women in this study also found the overall health as the worst amongst the assessed domains.
Research conducted by Professor Horst-Sikorska et al. showed that osteoporosis causes limitations in patients’ physical activity, pain and depressed mood, fatigue and insomnia [24]. The study showed that studied women also indicate limited physical and mental activity. According to the study conducted by Vujasinocić et al. in which authors were using the Qualeffo-41 scale, it was demonstrated that women with osteoporosis indicated much worse functioning in every field of the scale [25]. This research confirms that in addition to pain, general health, social and mental activity are assessed as worst by the surveyed women.
In a study conducted in Japan among women with postmenopausal osteoporosis, it was shown that daily activities identified in the domains were equal to 0.2 Standardized Response Mean (SRM), while social activities and the attitude domain reached SRM levels close to 0. In the present study the domain of General Health perception reached the worst value [26]. Wilson S. et al. in order to identify variables that can affect the quality of life (HRQOL) in patients with or without fractures, performed the assessment of bone mineral density (BMD) before the diagnosis of osteoporosis. The mentioned patients with the assessment of BMD before the diagnosis of osteoporosis had reduced physical performance component summary (PCS). In patients without fractures, low BMD indicated a decline in the quality of life [27] . In the present study, it is not possible to refer to the BMD, since such data was not collected, but it can be concluded that the average value of the Qualeffo-41 scale indicates a poorer quality of life for women after fracture than for women who had not experienced fractures. However, statistical analysis revealed no significant differences in this respect. Using the data obtained from 55 women, similar to what was demonstrated in studies by other authors, in this study we confirmed good psychometric properties of the Polish version of Qualeffo-41. In their studies, Lips P. et al. [28] and Bączyk G. [29] also achieved a very high coefficient of reliability of α-Cronbach for measuring physical functioning.
Caputo E. L. and Costa MZ in the review of the literature found that when it comes to the quality of life in the domain of physical aspects such as muscle strength and balance, with the exception of two studies, all reported improved quality of life in the physical domain of the patients after treatment [30]. It is clear from this study that treatment improves quality of life, but especially in case of pharmacological treatment it is important to take your medicines as prescribed by your doctor. Haus D., et al., demonstrated that compliance of women in post-menopausal osteoporosis is weak, but the reduction in dosing frequency of drugs and patient education on the disease and its treatment may improve the compliance [31].
Conclusions
Based on the results obtained in a standardized detailed questionnaire for evaluation of the quality of life in osteoporosis - Qualeffo-41, we can confirm that Polish women with postmenopausal osteoporosis have a fairly low quality of life. Unsatisfactory relations between the domains of Qualeffo-41 in the treated patients indicate a need for improvement in several domains Qualeffo-41, i.e. general health perception, social function, pain and mental function. This result confirms one of the methods to evaluate quality of life, which should be monitored both at the beginning and during therapy, as evidenced by the work Caputo E.L. and Costa M.Z. Quality of life in the course of the treatment would allow for a thorough analysis of the areas that affect most on the deterioration of overall quality of life. The attempt to verify correlation between the place of residence, age, BMI, fractures and quality of life of patients has demonstrated essential statistical dependence of terms of age.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
- Grzechocińska B. The problems of menopause. Treatment options. Medycyna Rodzinna, 2004; 2:55-60. [Polish]
- Pertyński T, Stachowiak G. Menopause - the facts and controversy. Endokrynologia Polska, 2006;57,5:525-534. [Polish]
- Whitfield JF. What Is Osteoporosis? In: Madame Curie Bioscience Database [Internet]. Austin (TX): Landes Bioscience. http://www.ncbi.nlm.nih.gov/books/NBK6278/. Accessed: 01 February 2015
- National Osteoporosis Foundation: What is Osteoporosis? http://nof.org/articles/7. Accessed: 02 February 2015
- Cosman F, de Beur SJ, LeBoff MS, Lewiecki EM, Tanner B, Randall S, Lindsay R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporosis International, 2014; 25(10):2359-81, DOI 10.1007/s00198-014-2794-2
- Głuszko P, Lorenc RS, Karczmarewicz E, Misiorowski W, Jaworski M. Polish guidelines for the diagnosis and management of osteoporosis: a review of 2013 update. Pol. Arch.Med. Wewn.2014;124:255-263
- Marcinowska-Suchowierska E, Tałałaj M, Kapuściński P. Osteoporosis: to whom threatens, how to avoid. PZWL, Warsaw, 2002. [Polish]
- Marcinowska-Suchowierska E, Tałałaj M, Kapuściński P, Dębski R, Chmielewski D. Osteoporosis. Diagnosis, prevention and treatment. PZWL, Warsaw, 1999. [Polish]
- Napiórkowska L, Franek E. Old age osteoporosis. Endokrynologia Polska, 2009; 60, 2: 110-114. [Polish]
- Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet, 2002; 359:1761-1767
- Jasiak-Tyrkalska B, Czerwiński E. Proceedings physiotherapy after osteoporotic fractures. Publisher Medsportpress, 2006; 4(6), 8:388-394. [Polish]
- Badurski JE, Dobreńko A, Nowak N, Jeziernicka E, Daniluk S, Mrowiec A. Bialystok osteoporosis study-2: epidemiology of osteoporotic fractures and 10 year fracture risk assessment in population of women in Bialystok region by FRAX™ – WHO algorithm. Reumatologia, 2008; 46, 2:72-79. [Polish]
- Marcinkowska M, Wawrzyniak A, Horst-Sikorska W, Burchardt W. Quality of life in patients after hip fracture. Akademia Medyczna w Poznaniu oraz Szpital Miejski w Poznaniu Oddział Chirurgiczny. Poznań, 2005. [Polish]
- International Osteoporosis Foundation. http://www.iofbonehealth.org/
- Badia X, Díez-Pérez A, Alvarez-Sanz C, Díaz-López B, Diaz-Curiel M, Guillén F, González-Macias J. Spanish GRECO Study Group.: Measuring quality of life in women with vertebral fractures due to osteoporosis: a comparison of the OQLQ and QUALEFFO. Quality of Life Research, 2001; 10(4):307-17
- Bączyk G. Measuring the quality of life in patients with osteoporosis - an overview of general and specific scales to measure quality of life. Reumatologia, 2009; 47, 5:300–306. [Polish]
- Haładaj R, Pingot J, Pingot M. Quality of life assessment in patients with spinal radicular syndromes. Polish Medical Journal, 2015; XXXVIII (223):20-25
- Bianchi ML, Orsini MR, Saraifoger S. et al. Quality of life in post-menopausal osteoporosis. Health and Quality of Life Outcomes, 2005; 3:78-84
- Papaioannou A, Kennedy CC, Ioannidis G, Sawka A, Hopman WM, Pickard L, Brown JP, Josse RG, Kaiser S, Anastassiades T, Goltzman D, Papadimitropoulos M, Tenenhouse A, Prior JC, Olszynski WP, Adach JD. The impact of incident fractures on health-related quality of life: 5 years of data from the Canadian Multicentre Osteoporosis Study. Osteoporos Int 2009; 20:703–714. Doi: 10.1007/s00198-008-0743-7
- Czerwiński E. Osteoporoza. Problem interdyscyplinarny. PZWL, Warszaw, 2015. [Polish]
- Abimanyi-Ochom J, Watts JJ, Borgström F, Nicholson GC, Shore-Lorenti C, Stuart AL, Zhang Y, Iuliano, Seeman E, Prince R, March L, Cross M, Winzenberg T, Laslett LL, Duque G, Ebeling PR, Sanders KM. Changes in quality of life associated with fragility fractures: Australian arm of the International Cost and Utility Related to Osteoporotic Fractures Study (AusICUROS). Osteoporos Int 2015; 26:1781–1790. Doi: 10.1007/s00198-015-3088-z
- Ström O, Borgström F, Zethraeus N, Johnell O, Lidgren L, Ponzer S, Svensson O, Abdon P, Ornstein E, Ceder L. Thorngren KG, Kernbo I, Jönsson B. Long-term cost and effect on quality of life of osteoporosis-related fractures in Sweden, Acta Orthopaedica, 2008; 79:2, 269-280. doi: 10.1080/17453670710015094
- Bączyk G, Opala T, Klejewski A, Tesarska B. Assessment of the women with osteoporosis fractures and without vertebral fractures of the spine based on the Polish version of Qualeffo-41. Chirurgia Narządów Ruchu i Ortopedia Polska, 2010;75 (3):172-177. [Polish]
- Horst-Sikorska W, Bryl N, Król I. What to look for in order to effectively cure patients with osteoporosis? What is the problem: the choice of the drug, or the maintenance of patient persistence in its use? Geriatria, 2011;5:207-211. [Polish]
- Vujasinović – Stupar N, Radunović G, Smailji M. Quality of life assessment in osteoporotic patients with and without vertebral fracture. Medicinski Pregled, 2005;58(9-10):453-458. [Serbian]
- Urushihara H, Yoh K, Hamaya E, Taketsuna M, Tanaka K. Responsiveness of the Japanese Osteoporosis Quality of Life questionnaire in women with postmenopausal osteoporosis. Health Quality of Life Outcomes. 2014; 12(1):178. doi:10.1186/s12955-014-0178-0
- Wilson S, Sharp CA, Davie MW. Health-related quality of life in women referred for bone density assessment: relationships with bone mineral density, fracture and co-morbidity. Quality of Life Research, 2015;24:1235-1243. doi 10.1007/s11136-014-0851-0.
- Lips P., Leplège A. Development and validation of a quality of life questionnaire for patients with vertebral fractures; Qualeffo-41. Quality of Life Research, 2000; 9:763-766
- Bączyk G, Opala T, Kleka P. Quality of life in postmenopausal women with reduced bone mineral density: psychometric evaluation of the Polish version of QUALEFFO-41. Arch Med Sci 2011; 7, 3:476-485
- Caputo EL, Costa MZ. Influence of physical activity on quality of life in postmenopausal women with osteoporosis. Revista Brasileira Reumatologia, 2014; 54(6):467-73. doi: 10.1016/j.rbr.2014.02.008. [Portuguese]
- Huas D, Debiais F, Blotman F, Cortet B, Mercier F, Rousseaux Ch, BergerV, Gaudin AF, Cotté FE. Compliance and treatment satisfaction of post menopausal women treated for Osteoporosis. Compliance of osteoporosis treatment. BMC Women's Health, 2010; 10:26, http://www.biomedcentral.com/1472-6874/10/26, Accessed: 23 May 2013

